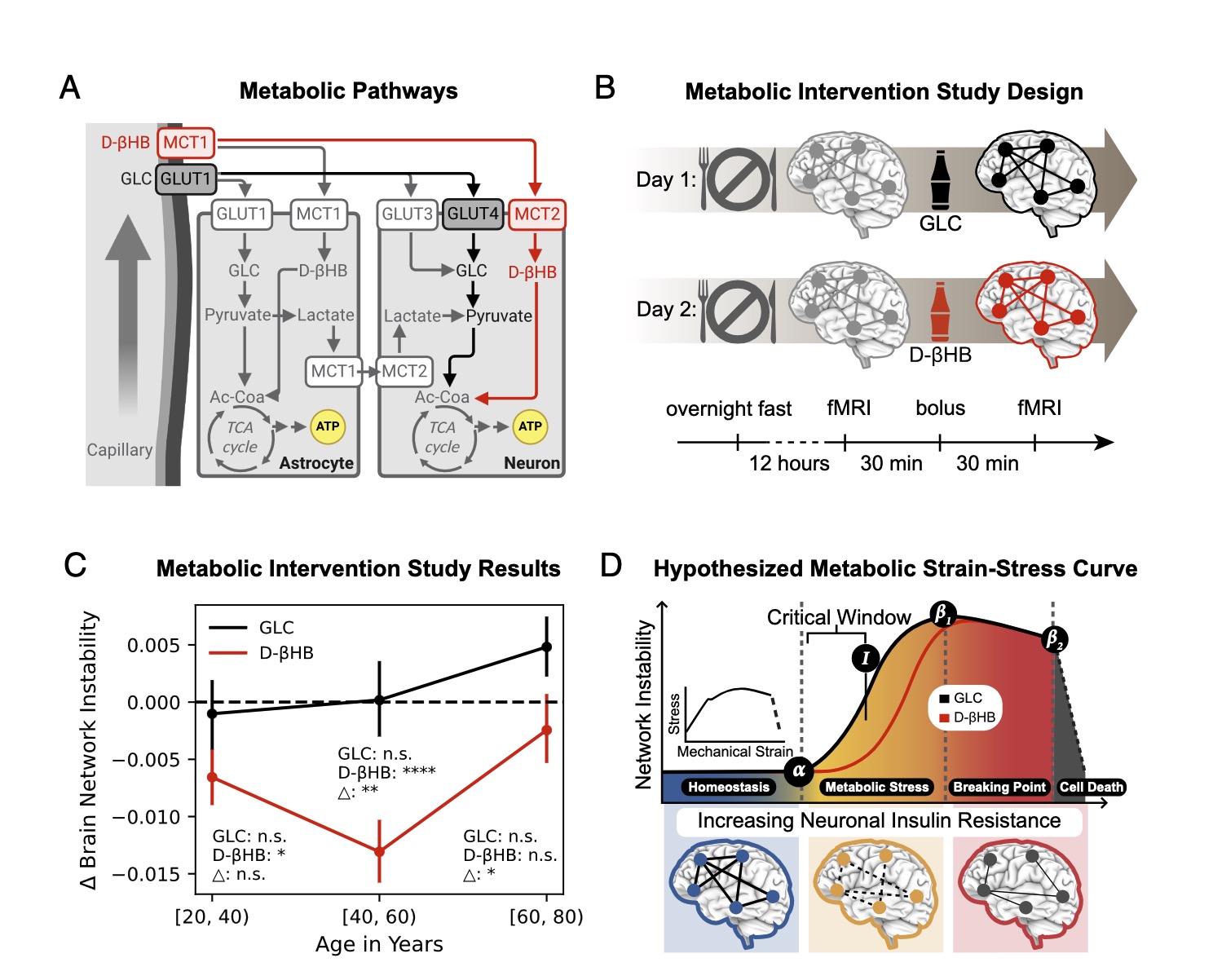
Age-related cognitive decline is associated with metabolic, vascular, and inflammatory changes, making it challenging to distinguish primary causes from secondary (downstream) effects. This study demonstrates that brain aging follows a specific progression, with the first stage occurring in middle age and coinciding with increased insulin resistance. Moreover, we show that brain areas that age fastest are also those most vulnerable to neuronal insulin resistance. Importantly, we find that administering ketones, which can fuel neurons while bypassing insulin resistance, reverses brain aging effects. However, this intervention is only effective when provided early enough for neurons to remain viable. These findings contribute to our understanding of brain aging mechanisms and suggest neurometabolic strategies for targeted early intervention in preventing age-related cognitive decline.
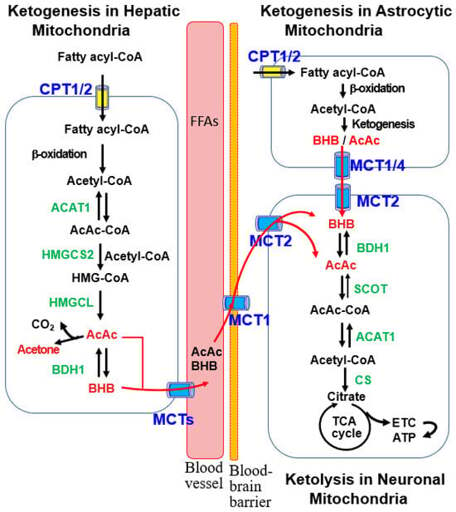
Understanding the key drivers of brain aging is essential for effective prevention and treatment of neurodegenerative diseases. Here, we integrate human brain and physiological data to investigate underlying mechanisms. Functional MRI analyses across four large datasets (totaling 19,300 participants) show that brain networks not only destabilize throughout the lifetime but do so along a nonlinear trajectory, with consistent temporal “landmarks” of brain aging starting in midlife (40s). Comparison of metabolic, vascular, and inflammatory biomarkers implicate dysregulated glucose homeostasis as the driver mechanism for these transitions. Correlation between the brain’s regionally heterogeneous patterns of aging and gene expression further supports these findings, selectively implicating GLUT4 (insulin-dependent glucose transporter) and APOE (lipid transport protein). Notably, MCT2 (a neuronal, but not glial, ketone transporter) emerges as a potential counteracting factor by facilitating neurons’ energy uptake independently of insulin. Consistent with these results, an interventional study of 101 participants shows that ketones exhibit robust effects in restabilizing brain networks, maximized from ages 40 to 60, suggesting a midlife “critical window” for early metabolic intervention.
Full Paper - https://doi.org/10.1073/pnas.2416433122
.