this post was submitted on 23 Oct 2024
26 points (100.0% liked)
Transfem
3417 readers
1 users here now
A community for transfeminine people and experiences.
This is a supportive community for all transfeminine or questioning people. Anyone is welcome to participate in this community but disrupting the safety of this space for trans feminine people is unacceptable and will result in moderator action.
Debate surrounding transgender rights or acceptance will result in an immediate ban.
- Please follow the rules of the lemmy.blahaj.zone instance.
- Bigotry of any kind will not be tolerated.
- Gatekeeping will not be tolerated.
- Please be kind and respectful to all.
- Please tag NSFW topics.
- No NSFW image posts.
- Please provide content warnings where appropriate.
- Please do not repost bigoted content here.
This community is supportive of DIY HRT. Unsolicited medical advice or caution being given to people on DIY will result in moderator action.
Posters may express that they are looking for responses and support from groups with certain experiences (eg. trans people, trans people with supportive parents, trans parents.). Please respect those requests and be mindful that your experience may differ from others here.
To make such a request, at the start of the body of your post, not in the title, the first line should look like the this: [Requesting Engagement from _________]
Some helpful links:
Support Hotlines:
- The Trevor Project // Web chat, phone call, and text message LGBTQ+ support hotline.
- TransLifeLine // A US/Canada LGBTQ+ phone support hotline service. The US line has Spanish support.
- LGBT Youthline.ca // A Canadian LGBT hotline support service with phone call and web chat support. (4pm - 9:30pm EST)
- 988lifeline // A US only Crisis hotline with phone call, text and web chat support. Dedicated staff for LGBTQIA+ youth 24/7 on phone service, 3pm to 2am EST for text and web chat.
founded 2 years ago
MODERATORS
Sublingual results in some still being swallowed, so one concern is about putting really high doses on the liver. There is also just the logistical difficulty of dosing frequently enough to keep your levels high enough, there is less margin for error.
Why not injections for monotherapy?
What about patches? That should spread it out.
What I've heard about patches is that it can be difficult to get your estrogen high enough with them (for monotherapy at least). I've also heard other problems like rashes, the patches falling off too early (and being expensive to replace), and needing too many to make monotherapy reasonable.
Again, why not injections?
In my opinion, injections are the gold standard. I just wanted to know if sublingual monotherapy was a possibility and if anybody had accomplished it.
It looks like some people have tried it with doses like 6 - 8 mg / day: https://old.reddit.com/r/AskMtFHRT/comments/k6lkyi/can_you_effectively_do_estrogen_monotherapy_on/
Still, it seems inadvisable. Just because you can doesn't mean you should. 😄
Thank you for the link!
Just copy pasting my notes from that link:
All at once, I don't want to stab myself, easier to put one on twice a week so I don't forget when lazy/tired. ESTRADIOL 0.1 MG PATCH (2/WK) is what I have.
One 0.1 mg patch isn't enough for monotherapy, but you could try multiple patches for monotherapy. What are you estradiol blood levels like with that dose?
I don't like stabbing myself either, but the benefits of injections outweigh those concerns (and I have done a lot to mitigate my needle phobia).
Well my hormones were off before I started and I'm post op now. My T before starting was 375 and my Estrogen total was 250. Now my T is 4 and my ESTRADIOL (E2) is 40
oh interesting, yeah - I am pre-op, so I am relying on monotherapy to suppress my T.
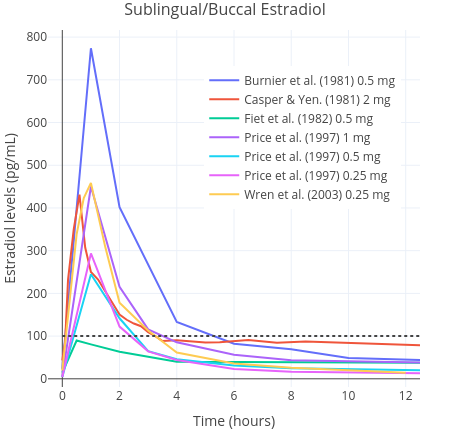
I just started HRT, Oral 2MG estradiol. I was just curious because I know that most of the sublingual meds are supposed to go directly into your blood stream and what heads to your liver should be minimal, as opposed to oral where the dose has to be high enough to pass through your liver.
I think I'm willing to pop them like tic tacs if needed.
Sublingual might have better absorption than oral, but that isn't saying much and you are still swallowing some of the dose. I still think the dose you would need to do monotherapy is more than is reasonable for oral or sublingual routes of administration.
Also, it's not just how many pills you would need to take to keep up your levels, but the exact timing. It also means all day you are constantly having sharp increases and decreases in your hormone levels. It's impractical for lots of reasons.
Injections are ideal for monotherapy, but if that's not an option I would stick to more typical doses of sublingual estrogen and an anti-androgen (though the anti-androgens can have side effects). Patches and gel are better for absorption than oral (most of the estrogen is absorbed by the liver, little of your dose gets into the bloodstream - it's really the worst route of administration), but they have their own logistical problems.
I highly recommend reading this: https://transfemscience.org/articles/transfem-intro/